Esophageal lesions
Where is the lesion?
(Mucosal, submucosal or extraluminal) How can you tell? What is the DDX for a lesion affecting the esophagus in that location?
(Mucosal, submucosal or extraluminal) How can you tell? What is the DDX for a lesion affecting the esophagus in that location?

Answers
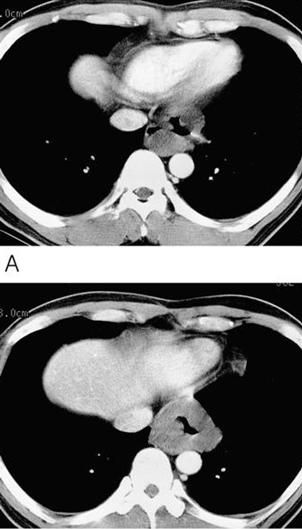
Esophageal Mass: Leiomyoma
Approach to UGI Masses
Approach to UGI Masses
- Location w.r.t. lumen
Intramural/submucosal – maintains mucosal pattern, obtuse angles - Extraluminal – mass effect, obtuse angles
- Intraluminal/mucosal – filling defect, acute angles
- Benign or malignant appearance:
- Benign – smooth gradual transitions
- Malignant – irregular, abrupt transitions, overhanging margins
- Location in ugi tract
Leiomyoma
- Finding: smooth soft tissue intramural mass that may calcify, ulcerate, and commonly has an exophytic component.
- Most common tumor of esophagus (50%).
- GIST includes leiomyoma and leiomyosarcoma.
- These tumors can be seen anywhere in the GI tract. About 50-70% of GISTs occur in the stomach; 33%, in the small bowel;5-15%, in the rectocolon; and only 1-5%, in the esophagus.
- DDX: lyphoma, sarcoma, carcinoma, mets.
- Usually assymptomatic, but can ulcerate, bleed, or undergo malignant transformation.
Esophageal filling Defects
Tumors
Benign:
Submucosal – leiomyoma, fibroma, lipoma
Tumors
Benign:
Submucosal – leiomyoma, fibroma, lipoma
Mucosal – Papilloma, polyp(adenomatous,postinflammatory,giant fibrovascular)
Malignant:
submucosal – Lymphoma, mets, leiomyosarcoma, GIST
Mucosal – Carcinoma-> adenocarcinoma, SCC, verrucoid Varices – uphill, ownhill
Extrinsic lesions – tumors, congential cysts(bronchogentic, duplication), osteophytes, enlarged nodes, abberent or enlarged vessels
Foreign bodies
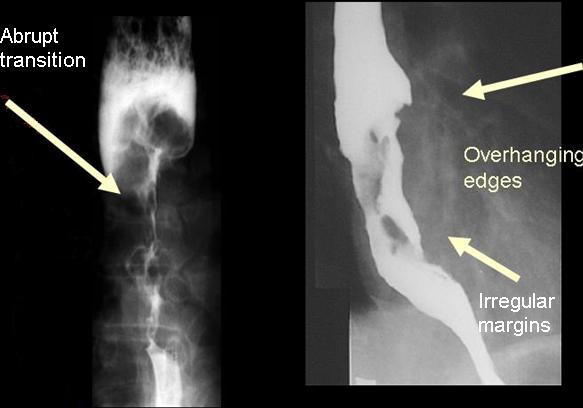
Distinguishing Features of Esophageal carcinoma
Risk factors – reflux, alcohol, caustics, achalasia, head and neck cancers.
90% SSC, 10% adenocarcinoma(associated with Barret’s)
Risk factors – reflux, alcohol, caustics, achalasia, head and neck cancers.
90% SSC, 10% adenocarcinoma(associated with Barret’s)
No comments:
Post a Comment